Registered Residential Customers
Manage Your Home Services
Zika is a virus of the genus Flavivirus and is closely related to dengue, yellow fever, Japanese encephalitis and West Nile viruses. It was first isolated from a captive rhesus monkey in the Zika forest in Uganda in 1947. It was first isolated from a mosquito, Aedes africanus, in 1948.
The disease caused by the virus is also called Zika and alternatively Zika fever or Zika virus disease.
This article covers the following topics:
In 1952, the first human cases were found in Uganda and the United Republic of Tanzania through the detection of antibodies in blood serum. The first known human infection was in 1954, after which it was rarely reported, with only 16 human cases reported, in Nigeria, Uganda and then Indonesia up to 1981. At that time it was suggested that the lack of reported cases was due to its clinical similarity to dengue and chikungunya.
The first large outbreak was in 2007 on the Pacific island of Yap, in the Federated States of Micronesia, later identified as a strain from Southeast Asia. The suspected vector in this rural outbreak was a local mosquito species, Aedes hensilli.
Zika spread to French Polynesia in 2013 and for the first time became an urban epidemic, where the main vector was Aedes aegypti. It spread to Brazil in 2015, when the country was suffering a dengue outbreak, carried by the same mosquito. After this it spread rapidly around tropical South America and the Caribbean.
By June 2016 it had been reported in 63 countries or territories and was associated with over 1500 cases of microcephaly or central nervous system (CNS) malformations. The number of countries and territories with infections had risen to 84 by early 2017, according to WHO.

Yellow fever mosquito, Aedes aegypti
Zika can be transmitted:
The virus is primarily spread through bites of infected Aedes species of mosquito, including Ae. aegypti and Ae. albopictus. It therefore has the potential to spread anywhere these mosquitoes can survive (see figure 1).
The mosquitoes bite in the daytime, unlike most mosquito species, so it is important to take precautions when going out in infected areas.
A pregnant woman who is infected with the Zika virus can pass it to her foetus during pregnancy as the virus can cross the placental membrane.
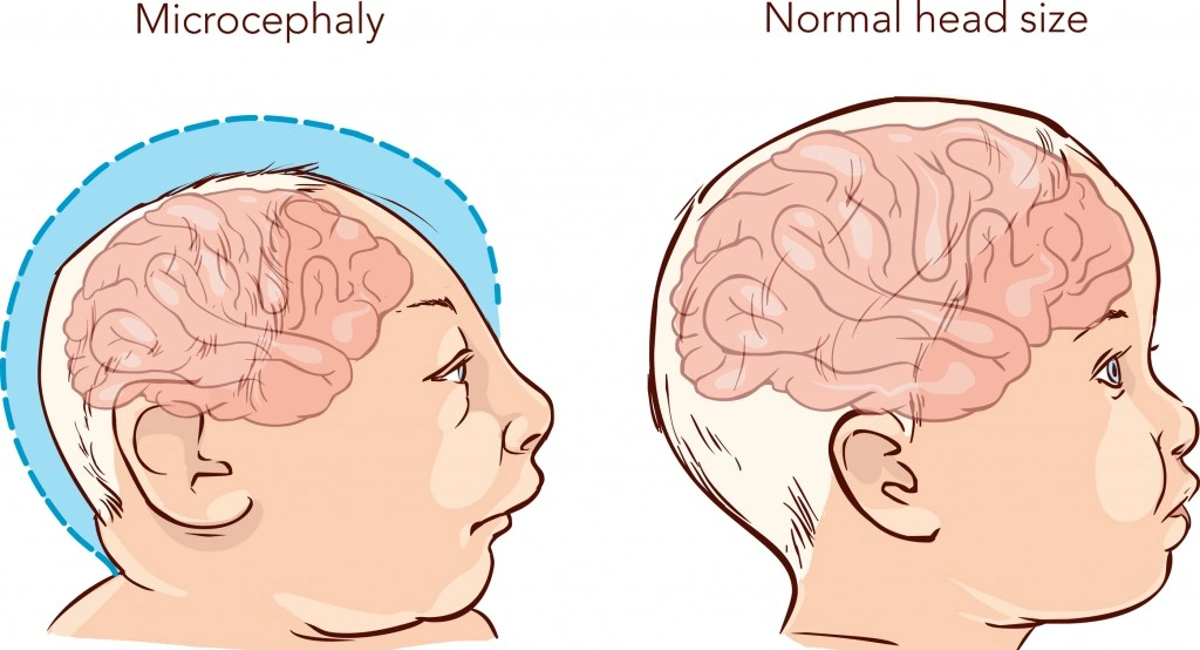
The Zika virus can cause microcephaly and other severe brain defects in the foetus. Research is still ongoing to study other health problems.
See more information about Zika regarding women and pregnancy.
The Zika virus can be transmitted from an infected man to his sex partner before the symptoms show, when he has symptoms and after the symptoms have gone.
WHO updated its recommendations in June 2016 to advise travellers returning from areas with Zika virus to use a condom for at least 8 weeks after returning, but if Zika virus symptoms occur during that period to use condoms or refrain from sex for at least 6 months.
The US CDC reports that there have been multiple reports of Zika being transmitted by blood transfusion in Brazil.
The virus was also found in a small proportion of blood donors in French Polynesia during an outbreak.
According to CDC there have been several cases of Zika transmitted in a laboratory and healthcare settings, but the routes of transmission have not been clearly identified.
Source: Mapping global environmental suitability for Zika virus. eLife 2016;5:e15272
Zika was declared a Public Health Emergency of International Concern by WHO in February 2016. In June 2016, the WHO published an 18-month strategy to guide the international actions against the Zika infection, its complications and consequences.
The major focus has now moved from mainly mosquito control to an integrated approach combining risk communication, integrated vector management, sexual and reproductive health counselling and services, health education and care.
“Much has been learned about Zika virus infection... the response now requires a unique and integrated strategy that places support for women and girls of childbearing age at its core.”
— Dr Margaret Chan, WHO Director-General (2016)
(from WHO Global response page)
The major areas of outbreak were in the northeast of Brazil and poorer countries of the region, where “poverty, poor infrastructure, and lack of access to health services are rampant, and the penetration of Aedes aegypti is high.” (The Lancet Global Health)
Zika is not often seen in developed urban areas and the air conditioned shopping malls and hotels of major cities, therefore most residents and travellers in these areas have a low risk of infection.
The incubation period for Zika virus is not known, but is thought to range from a few days to a week.
A large proportion of people infected have no or mild symptoms. Only one in five infected people develop symptoms and people very rarely die from the disease. A Zika infection generally lasts for 2-7 days.
The most common symptoms of a Zika virus infection are:
The symptoms are similar to dengue and chikungunya, which are also transmitted by Aedes mosquitoes, so could be confused with them.
Research published in the journal Nature in 2016 suggested that the rapid expansion in Zika infections in South America in 2015 and 2016 may have been due to previous exposure to dengue virus. It was already known that one dengue infection weakened the immune response to a second infection of the same strain.
It has recently been shown in the lab that Ae. aegypti can carry Zika and chikungunya at the same time and transmit both viruses in saliva. Some patients in Nicaragua who tested positive for dengue, chikungunya or Zika were also found to be infected with one of the other viruses.
A diagnosis is based on a person’s symptoms and their recent history of travel and potential mosquito bites. A blood or urine test can confirm infection with the Zika virus. These require labs with the capability to perform the appropriate PCR tests, require technical expertise, are relatively expensive and take several weeks.
Rapid diagnostic tests suitable for use in low-resource and remote areas are reported to be under development, but are not available for general use yet.
In the US, the FDA has issued an Emergency Use Authorization (EUA) for two new diagnostic tools for Zika virus (the Zika MAC-ELISA and Trioplex Real-Time RT-PCR Assay), but only qualified laboratories are allowed to use them.
The Zika virus is transmitted to people mainly through bites from infected Aedes aegypti mosquitoes but can also be transmitted by Ae. albopictus. As mentioned above, it can occur in other species. In Africa it was originally found in Ae. africanus and in Micronesia Ae. hensilli was thought to be responsible.
Ae. aegypti
Ae. aegypti, the yellow fever mosquito, is thought to have originated in Africa and transported throughout tropical, subtropical and parts of temperate areas of the world through global trade and shipping activities. It relies largely on human habits to provide breeding grounds — in small containers of water and standing water.
It cannot fly far to obtain a blood meal and feeds almost exclusively on humans (termed anthropophilic), so needs to be close to human habitation. Unlike most mosquito species, it feeds mainly during the daytime. Ae. aegypti is highly effective in transmitting several arboviruses that cause serious illnesses in humans: dengue, chikungunya, Zika and yellow fever.

Figure 2. Global map of the predicted distribution of Ae. aegypti,/i>. The map depicts the probability of occurrence (from 0 blue to 1 red).
Source: Kraemer et al. eLife 2015;4:e08347. DOI: 10.7554/eLife.08347
Ae. albopictus
Ae. albopictus, the Asian tiger mosquito, originated in tropical Asia and has also been transported around the world into tropical, subtropical and some temperate areas through international trade. It is believed that imports of used tyres introduced it to the US.
Ae. albopictus can survive a wider temperature range and cooler temperatures than Ae. aegypti, which gives it a greater ability to survive and spread in areas with temperate climates, including Europe and more extensively than Ae. aegypti in the US. It can feed on animals and humans so can live in urban areas near humans and in woodland.

Figure 3. Global map of the predicted distribution of Ae. albopictus. The map depicts the probability of occurrence from 0 blue to 1 red.
Source: Kraemer et al. eLife 2015;4:e08347. DOI: 10.7554/eLife.08347
Aedes mosquito life cycle
The Aedes mosquito life cycle consists of the following stages:

There is no vaccine or specific treatment for the Zika virus.
A Zika infection is usually mild and does not require any treatment, but WHO recommends that people with the disease should:
Prevention of Zika is carried out at two levels: activities for government and non-government agencies at the population level, and personal protection to prevent mosquito bites.
With the publication of the latest WHO strategy (June 2016), the global strategy for the prevention of Zika at the wider level includes:
Detection
Prevention
Personal protection involves avoiding high-risk places and prevention of mosquito bites, for example, using insect repellent, wearing long sleeves and trousers, and staying in places with window and door screens.
The Zika outbreaks in French Polynesia and Brazil have been associated with congenital malformations in babies and neurological and autoimmune complications, in particular, microcephaly and Guillain-Barré syndrome.
The World Health Organization maintains a Q&A website on the Zika virus and its associated complications with the most up to date information on this rapidly developing topic.
CDC factsheet on the Aedes lifecycle
Insect-borne diseases pose immense health & economic threats